Aravind
Founded: 1976, Tamil Nadu, India
Tags
Story
Today, the Aravind Eye Care System is a network of hospitals, clinics, community outreach efforts, factories, and research and training institutes in South India that has treated 65 million patients and has performed 7.8 million surgeries. Its surgeons are 5 times more productive than the industry standard. In 2017 to 2018 the group performed 60% of the total volume of surgeries performed by the entire NHS, at one hundredth of the cost, and less than half the rate of complications.
Aravind established its first overseas venture in Nigeria, with a partnership with the Tulsi Chanrai Group and will celebrate its 2 year anniversary in January 2020.
Business Model
Twelve million people are blind in India, the vast majority of them from cataracts, which tend to strike people in India before 60 — earlier than in the West. Blindness robs a poor person of his livelihood and with it, his sense of self-worth; it is often a fatal disease. A blind person, the Indian saying goes, is “a mouth with no hands.”
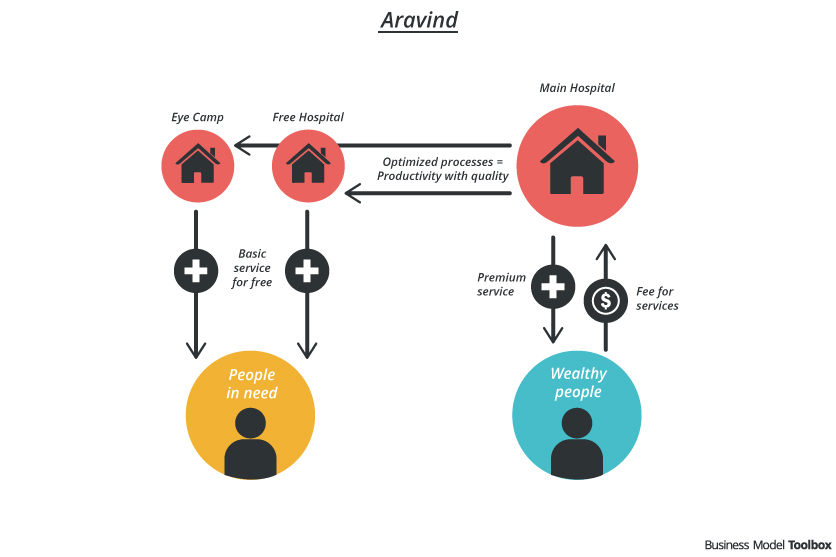
Aravind Eye Care, the largest and most productive eye care facility in the world, offers free eye care and surgery to 50% of its patients. Therefore, they run two different kinds of hospitals – the Main Hospital and the Free Hospital. The Free Hospital focuses on offering basic but quality service for people in need: No bed is provided to the patients but a small pillow and a coir mat.
The Main Hospital functions like a regular ophthalmology hospital. All patients admitted here pay for the hospital’s services. The hospital offers different classes of rooms with different levels of privacy and comfort. Treatment performed in the Main Hospital varies from simple treatments to extremely complex surgeries like retina detachment repair.
Established in 1976, Dr. Venkataswamy started Aravind Eye Hospital with the mission to eliminate needless blindness. By adopting an efficient operation procedure like a fast-food chain assembly line, Aravind manages to keep its cost low without compromising the quality. A majority of its services is done free of charge.
“Achieving scale and improving productivity has enabled us to keep costs down and treat hundreds of thousands of patients each year. It has allowed us to give back to society, to the communities.” Dr Srinivasan, Director of Projects, Aravind Eye Care System (source: McKinsey “Driving down the cost of high-quality care—Lessons from the Aravind Eye Care System”)
Aravind does 60% more eye surgeries than the UK National Health System, at one-thousandth of the cost. Efficient operation procedures and a high volume of patients enable this.
The hospitals operate like an assembly line with a minimum turnaround time. (No-Frill Business Model). This ensures the surgeons to be able to carry out a significantly larger number of surgeries than is possible normally. Batches of patients would be prepared before surgery and bandaged afterwards by Aravind-trained nurses. After completed surgery, surgeons immediately move to the next operating table where a second support team is waiting with the patient ready to be operated. This results in tremendous efficiency. Aravind doctors can do more than 2,000 surgeries a year, while the average at other Indian hospitals is around 300.
To support the high volume, Aravind reaches the masses through eye camps, which take place in rural and semi-urban areas. At the camp, patients are screened and those found suitable for surgery are prepared. Another major factor that bring down costs significantly is that Aravind has its own factory producing intraocular lenses.
“Aravind is not just a health success, it is a financial success. Many health non-profits in developing countries rely on government help or donations, but Aravind’s core services are sustainable.” NY times Opinioator: A Hospital Network with a Vision.
Efficient operation procedures and a high volume of patients enables Aravind to generate a high EBITDA.
The revenue generated from the Main Hospital enables the Free Hospital to provide free eye treatment to the poorer section of the society. Patients are brought in from eye camps for free treatment. (Get one – give one business model)
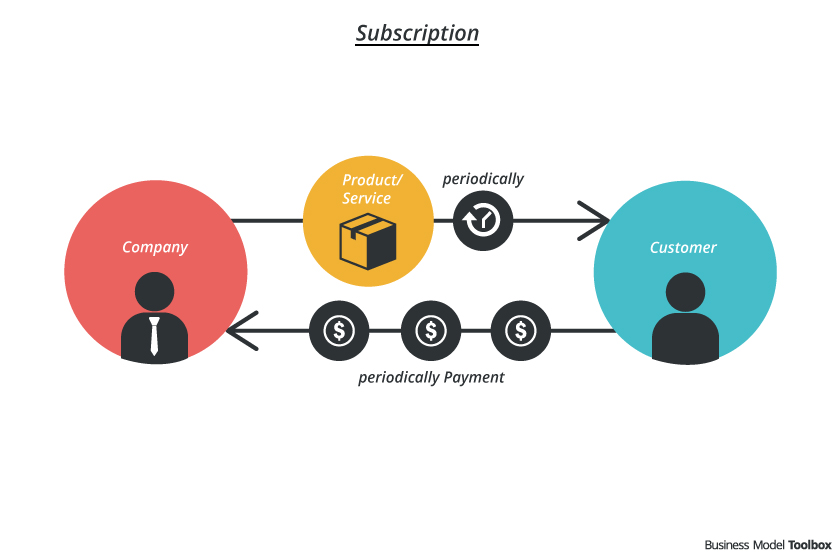
Patients at the Main Hospital can choose between different classes of rooms, with different levels of privacy and facilities and consequently different price levels. (Add on business model)
Efficiency resulting from the innovation operation procedure is definitely a key strength of Aravind Eye Care. In addition, “it is not leadership in the sense of organizing and making it work. It’s leadership that comes from empathizing with the community,” Dr. Venkataswamy said in an interview with the NY Times. “Never restrict demand. Build your capacity to meet the demand.”
The Aravind Eye Care network includes a network of eye care facilities, a postgraduate institute, a management training and consulting institute, an ophthalmic manufacturing unit, a research institute, and eye banks. Its eye care facilities include 14 eye hospitals, 6 outpatient eye examination centers, and 80 primary care facilities.
Applied Patterns
Challenges
Transportation is a problem for some of the selected patients from eye camps. They may not be able to travel to the hospital for surgery or to stay away from home for long periods, hence lead to a drop in the number of patients accepting surgery.
The flow of patients would be much larger immediately after an eye camp and being much less at other times. The hospital was overcrowded while it operated much below is capacity at other times.
Patients are required to come to the hospital for treatment. The camp could not be conducted at a location that was very far from the hospitals.
Positive Impact
- Reduce number of blindness among poor population
- Enable longer economic productivity in poor regions by improving health condition (vision).
- Lower the cost of lenses production
- Highly scalable model that can be expanded to other regions and countries
Negative Impact
Resources
- Website: Aravind
- McKinsey: Driving Down the cost of high-quality care Lessons from the Aravind Eye care system
- FastCompany: And Then There’s Dr. V
- New York Times Opinioator: The Hospital Network with a vision
- Harvard Business School: Aravind Eye-Care System – McDonaldization of Eye-Care
It is very inspiring business model & adopting such models can solve a lot of our societal problems in a sustainable manner.